Sales: 508-836-2700
Published on Wednesday May 17, 2017
Physicians work in medicine, not farming, but sometimes the data they need is hiding in silos scattered all over the healthcare field. eClinicalWorks’ own Tushar Malhotra discusses what is being done to solve today’s interoperability challenges, giving providers the data they need, on demand and at the point of care.
“We are not just saying ‘Yes, we are supportive of the idea.’ We are actually doing it for them. We are seeing real world exchanges happening, and that’s a key differentiator for eClinicalWorks. That has helped put us in the leading quadrant of EHR vendors when it comes to interoperability.”
Tushar Malhotra, eClinicalWorks interoperability team

Topics From This Episode
Interoperability Solutions
EHRs are nearly universal in U.S. medical practices, but a given patient’s data can be scattered among their primary care doctor, specialists, clinics, and hospitals. To ensure quality care and patient safety, physicians need to reach across diverse EHRs and institutions to obtain complete medical histories. That means interoperability. Through the Carequality and CommonWell interoperability frameworks, eClinicalWorks provides clients with the most complete visibility of each patient’s record.

Automated query
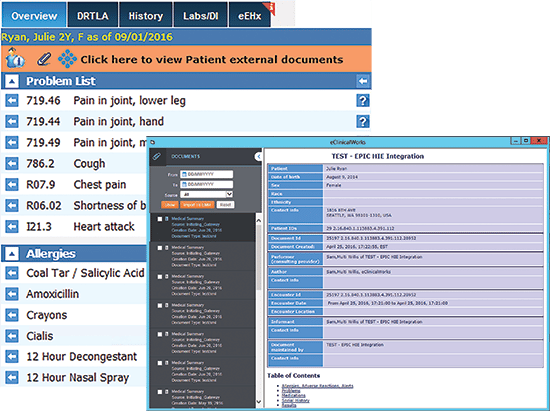
Interoperability itself isn’t new, but for years providers and organizations have been reliant upon point-to-point interfaces. While effective, they are time consuming and expensive to build, and deliver data from just a single source. Now, as soon as a patient checks in with their medical provider, the eClinicalWorks EHR queries the Carequality and CommonWell frameworks for that patient’s data from all locations, and displays it in the Interactive Clinical Wizard (Right Chart Panel).
On-Demand Activation
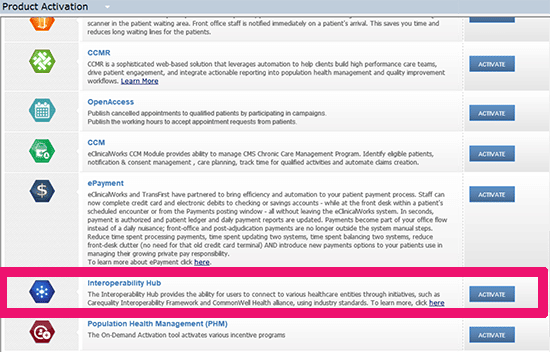
While the technology behind interoperability is complex, using it is simple. eClinicalWorks offers clients on-demand activation (ODA) of CommonWell and Carequality through the Interoperability Hub on the ODA screen within the EHR. The practice administrator or physician simply accepts the terms and conditions for Carequality and/or CommonWell and within a few days data can begin flowing.
Track allergies, meds and more
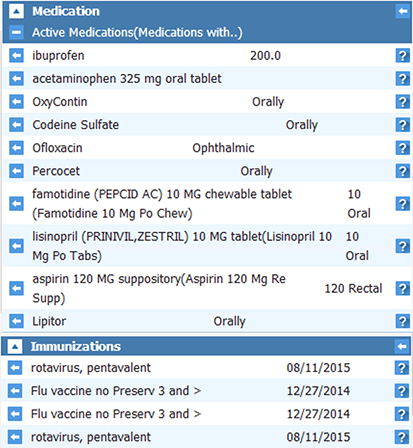
eClinicalWorks makes sure that providers receive that data in the most usable form possible. Critical patient safety data, including allergies, medications, and immunization records, is discretely importable. And if a provider wants to see specific data elements such as past lab results, physicals, or hospital discharge summaries, they can access that information with a single additional click. And the information exchange is bi-directional, allowing other providers to query eClinicalWorks practices.
Subscribe to our podcast easily with your smartphone on iTunes®.
Transcript:
Adam: They say that no man is an island, but until recently, the same could not be said of patient information which had been frequently isolated and segmented among various settings of care. I’m Adam Siladi with the eClinicalWorks podcast and today we’ll be speaking about the advances in the interoperability space. Joining me to speak with us about that today is Tushar Malhotra from our interoperability team. Tushar, thank you so much.
Tushar: Thank you for having me.
Adam: Recently eClinicalWorks released a press release, talking about our partnerships with CommonWell and Carequality, two players in the interoperability space. Tushar, we’d like to learn a little bit more about what that really means and what clients can expect from that. But first thing’s first, let’s figure out what the context is – why do we need interoperability and what problem is it solving for our clients?
Tushar: I think you picked it up from the right place, where the problem exists that the data is in siloes all over the healthcare field right now. The patients are going to PCPs, they’re going to specialists, they’re going to the doctors in the hospital, or sometimes they end up in the ER. Different systems are being used across the board in those various care settings. What happens is that the patient data does not travel with the patient, the patient data tends to be siloed out, and that’s exactly the problem which these initiatives like CommonWell and Carequality are trying to solve. They’re trying to make sure that regardless of where the patient care is being given, the data flows with the patient. I’ll give you an example, so a patient was seen at the PCP’s office, and they found out that there was a critical drug allergy that this patient has. Now the patient ends up in the ER and the ER physicians don’t even know about that information. So that is a major gap in the care of the patient. Similarly, patient gets discharged from the hospital, the PCPs don’t even get to know about that. Duplicate tests are being ordered, expensive tests, like MRIs and CT scans are being ordered all the time, repeatedly, for that same patient because they don’t even know that this test has already been done in a different care setting.
Adam: Or, maybe because they have an incentive to order that additional duplicate test at this time that could be the case, as well.
Tushar: Exactly, and in the current day and age, where everything’s about pay-for-performance, I think it’s more important than ever to have this interoperability between the physicians so that they can control the cost of the riskier patients.
Adam: So, let’s take a step back, just for a quick moment, to ask one more question about the patient information that’s being exchanged. What do we find in scenarios where the patient may not have given consent, to share information from a certain setting of care, or maybe they have been in a certain setting of care and they want certain pieces of their information not to go to another provider?
Tushar: So that governance actually exists at the EMR level, so if the EMR is, let’s say, for a multispecialty clinic and there are certain visits which have been documented by a behavioral health physician or there have been some substance abuse in that type of data at the clinical visit, providers can actually mark those visits as private and not share them through these initiatives. So that opportunity exists, and even though the consent is on file for the rest of the patient record, certain parts of the patient record will be blocked from sharing.
Adam: Yes, Tushar, that’s right, we know through a recent legislation that providers are going to be expected to take on more of the control of the cost for the patient, often with the patient’s PCP, and without the information from those different sites, you know, providers often say it’s very difficult to track that information and take care of that. So it’s good to know that we’re hopefully going to see some more information flowing back and forth amongst that. Alright, Tushar, we know a little bit about why interoperability is important for patients and for providers, but that leaves vendors, right? Like eClinicalWorks. So why is it so important for vendors to start paying attention to interoperability, as well?
Tushar: So in the recent past, the 21st Century Cures Act was a new legislation that was passed, which puts a lot of spotlight on EHR interoperability, and trying to make sure that the private sector initiatives like CommonWell and Carequality are recognized for advancing interoperability in the healthcare industry. So, the work that the vendors are now trying to do is essentially partner up with either CommonWell or Carequality — eClinicalWorks happens to be a member of both — and connect our practices to pretty much any other entity which is part of these initiatives.
Adam: So eClinicalWorks is not only a member, but we’re a contributing member of these Carequality and CommonWell alliances. Tell us a little bit about what that means for our clients.
Tushar: Yeah, that’s a very important point, actually. There’s a difference being a general member, which supports the idea of interoperability, versus an actual implementer in the case of Carequality and a deploying member in the case of CommonWell. We are actually deploying these services for our clients, so if a customer comes and asks, we are not just saying “Yes, we are supportive of the idea,” we are actually doing it for them, we are seeing real-world exchanges happening and that’s a key differentiator for eClinicalWorks. That has helped us put in the leading quadrant of EHR vendors when it comes to interoperability.
Adam: So we’re not just interoperability groupies, we’re actually making things happen. What about the steps to get from a client who says, “OK, fine, I’ll do the interoperability bit,” to getting the actual data? What is the start to finish of signing up and then getting your information?
Tushar: Right. So it starts with an on-demand activation feature. So we have tried to make it really simple for the users, we have embedded that as interop hub on-demand activation on the EHR. The provider or the administrator, goes in there, accepts the terms and conditions, and they activate Carequality or CommonWell or both for their practice. The important term and condition which everyone should know, as an eClinicalWorks customer, is that we are providing the service at no cost for the next three years, so that’s a great advantage and it’s a great opportunity for the providers and clinics to get signed up as soon as possible.
Once they do that, the data can actually start flowing within a matter of three to four days, depending on what other entities are live on the network that they are participating in, which are in and around them, and what the consent model is that they have, and it also depends on whether the directory entries for that clinic have been added by the participating hospital on the other end. Once that happens, it’s actually a very automated workflow, as soon as the patient arrives in eClinicalWorks, behind the scenes we will go out and make a query for that patient and try to fetch the data back into eCW, and that data sits in the right chart panel of the eClinicalWorks Progress Note – problems, allergies, medications and immunizations are actually discretely importable. In addition to that, if there’s specific data elements like past lab results or history in physicals from a hospital visit or any discharge summary that the provider wants to see, all of that is accessible through one additional click, essentially. So it’s just very seamless, this entire information exchange, and it works bi-directionally, so if someone else wants to query an eCW practice, that can happen as well using these initiatives.
Adam: So we have a lot of details there, let’s just recap some of them for our listeners and our viewers. First, you said that you can activate Carequality or CommonWell connections via the on-demand tool in eClinicalWorks and you can start seeing information flowing in, in as little as three to four days. And of course, like you said, that depends on the other people on that network who are seeing your patients, if they haven’t seen your patient yet, there won’t be anything there. But I think one of the most interesting things that you shared was that the information is queried as soon as the patient is marked arrived in the eClinicalWorks system, so you don’t have to go out and connect to some sort of an interface or a hub, you don’t have to initiate a request on your side to get that information, it’s being done automatically for you. It’s kind of like when the patient used to arrive in the office and someone from the staff member would go grab their chart off the shelf and bring it to the doctor without being asked.
Tushar: Exactly. And that’s what’s happening in the real world at this point, the medical assistants or the staff at the clinic, they are prepping the charts ahead of time because this query has gone out, fetched the data, and a lot of the information that the providers need at the point of care is already being made available right there.
Adam: So, another thing that you mentioned that’s very important, is you started to talk about what happens to the data that the eClinicalWorks provider records in their Note, and how that’s dealt with. Let’s talk a little bit more about that scenario. So once the data is retrieved from these networks, used in the office setting, what happens then? Does the data go back to CommonWell or Carequality or some central hub somewhere? How is that treated?
Tushar: No, that’s the best part about CommonWell and Carequality, is that it’s entirely a federated model, what that means is there’s no concept of a central depository. Traditionally, if a practice has requested a connection to any of these initiatives, to any of the HIEs, they would have to build a point-to-point connection, and there will be a lot of time and effort that’s required. The end result was very regional in nature because they were only able to see data from certain participants who were actually participating in the HIE. This actually removes or changes all of that. We are essentially going out into the network, fetching the data from all different possible locations, and they could be from anywhere in the United States, as long as the patient has been given care at those other locations, and we bring that back into eCW, so it’s very seamless in that regard.
Adam: How are CommonWell and Carequality different? So, if I’m a provider who’s in my ODA tool, I’m given the choice – do you want to do Carequality or CommonWell — which one do I choose? How do I know? Maybe I don’t even have to, like you said before, but what’s the difference between the two?
Tushar: They’re both quite similar. There is a concept of a national record locator service, that’s the service which is provided by Surescripts – when that is coupled with Carequality, it actually equates to CommonWell. It’s the same thing being done, the only key difference, that I would say, is the patient validation step, which occurs in CommonWell, and does not occur in Carequality. So, the premise here is that Carequality will go ahead and make a query based on the demographics like last name, first name, date of birth, gender and ZIP Code. And if a match is found anywhere in the network, we’ll bring the data back. However, in CommonWell, there is one additional step. A match is found, but then we are asking the patient, at least once, at some point of care, it could be an eClinicalWorks setting or some other point-of-care setting, where we are asking the patient – ‘Are you sure that you went to this other location?’ If the patient says yes, only then a query is made, so there’s a slight difference there, but the end result is the same. The data is presented in the same way in eClinicalWorks. It’s presented to the users or consumed in the same way in the EHR, so everything stays the same, regardless of whether the query is going to Carequality or CommonWell entities. One more slight difference is the actual participant entities on the acute care side between Carequality and CommonWell. So, Cerner is part of CommonWell, whereas Epic is part of Carequality, and that could be your determining factor for any entity which is on eCW, trying to exchange data with Carequality versus CommonWell, depending on who their critical exchange partner is, do they happen to be on Cerner or Epic or some other acute care system?
Adam: So if I were a client and I went to the CommonWell or Carequality website, would I be able to see all of the different partners and figure out who I should connect with?
Tushar: Yes, exactly. So the CommonWell and Carequality websites provide you with the actual list of members who are deploying at any given time, so that information is right there, readily available for you.
Adam: So, among these two networks, Carequality, CommonWell, how many members do we have? What’s the reach and what could our clients reasonably expect when they’re looking for partners here?
Tushar: Right, so I’ll just give you some rough numbers on the two major vendors who are deploying either CommonWell or Carequality. Cerner is deploying CommonWell and they have about 100-acute care health systems that are live on the network. Epic, on the other hand, which is deploying Carequality, has about 180-odd customers that are live on the network. When I say a health system, it essentially could be multiple hospitals within the same health system. So, the actual number is close to 400 of acute care settings nationwide, which are live. So a great opportunity already exists for our clients to go ahead and get connected. And if we add to that, thousands of ambulatory sides, not just eClinicalWorks, but other vendors which are live on the network, it’s just a tremendous and really powerful network already.
Adam: And I’m sure those numbers are growing every day, more and more people being added to it. So, let’s talk about actually using this and if clients have been interested. So far they’ll probably want to know how to get started. Is there any kind of a version requirement for eClinicalWorks users?
Tushar: Yes, the version that the clients need to be is on SP1 C20, or higher, as long as they have that version, which, in fact, I think is a patient safety-recommended version from eClinicalWorks in any case – as long as they get that, they’re good to go for both these initiatives.
Adam: Of course, and if clients are unfamiliar with which version they have, or they can check, I’m sure they can talk to their SAM and ask that question there as well. And now from the eClinicalWorks standpoint, other than this podcast, of course, what is eClinicalWorks doing to help users get started?
Tushar: So, a few things that we are doing. First of all, first thing we are doing webinars twice a week, just to educate our customers on what these initiatives are and what they can learn from this and how they can get connected.
Adam: Are those free webinars?
Tushar: Those are free, yes. They’re free and they can sign up through the support portal for those webinars. We are also putting some videos, documentation like FAQs, user guides, and training manuals on how to use once they go live. And then the whole idea of on-demand activation in itself is really enhancing this for the providers because it’s not just that the client opens the case and then it sits in the queue for some time and then a project manager is assigned. It’s not a weeklong or month-long project. It’s actually a matter of a few clicks and they are live on the network. So embedding the technology to the level where a provider can activate CommonWell or Carequality using ODA, I think that has really helped making it easy in adopting these initiatives.
Adam: I’m sure that will remove some of the anxiety of getting started with a new initiative, and of course with all the education and everything, I’m sure they’ll be well-equipped for that. So, let’s talk about what’s coming up in the future. What’s on the roadmap for all this interoperability?
Tushar: Right, so in 2017, a big thing is going to be around FHIR, APIs, it’s also a requirement from the MU3 perspective, so a lot of work will be done in the next two or three quarters in making an open API, at least for the Common Clinical Data Set available to meet the Meaningful Use requirements, so a lot of work is going to be happening on that. From a CommonWell and Carequality perspective, we are working on many different things – one being that if a client is currently connected to an eHX or any other health information exchange, CommonWell and Carequality, so far, were not able to co-exist with them, so now we’re almost done with the development. That’s one big step forward. There are a big chunk of clients, like bigger communities, or those who are connected to a state or a public HIE or a REO, they would be able to connect with CommonWell and Carequality, as well. Then, in addition to that, we are working on making a facility-level filter, so that the scenario where I was explaining, if it’s a multi-specialty clinic, and they have behavioral health and some sensitive data in a specific facility, but they still want to participate in Carequality, we will give the entire facility data to be filtered out when a request comes in or goes out. So that’s another development that we are working on. In addition to that I think there are a couple more things that we are working on – one is a manual query, a functionality which does not exist as of now. That will be added, because sometimes the providers need to make a query on a patient outside the visit, like a telephone encounter. So we are planning to add that in the near future. And then we are also trying to support additional documentation types like the complete Progress Note or lab results data, packaged inside a CDA document, so that’s coming.
Adam: Well, it certainly sounds like there is a lot of stuff to work on. You better get to is after this. Thank you very much for the time you’ve taken to explain all this to myself and our viewers. If you’d like to watch any other of our eClinicalWorks podcasts, you can check them out on iTunes, YouTube or my.eclinicalworks.com. Of course my.eclinicalworks.com is where you can find all of that documentation and information that Tushar had mentioned, also check that out as well. Thank you everyone for watching. For the eClinicalWorks Podcast, I’m Adam Siladi, we’ll see you next time.
