Sales: 508-836-2700

Published on Thursday January 10, 2019
At the 2018 National Conference in Nashville, Tennessee, eClinicalWorks’ Brian Saal sat down with Jose Rocha, director of Neurosciences Corporation in Florida, to find out how First Choice Neurology’s many providers are using interoperability solutions to reduce costs and improve the continuity of care across dozens of practice locations. Now, with eClinicalWorks, the latest patient records are just a few clicks away — promoting better quality care and lowering the risk of physician burnout.
“It has worked out great for us, because it assists us to have at a moment all of the information — from not only from the hospital but also several other providers — available to us. And it reduces the medications being tried that were already tried by the patient, or repeating procedures.”
Jose Rocha, First Choice Neurology, Florida

Topics From This Episode
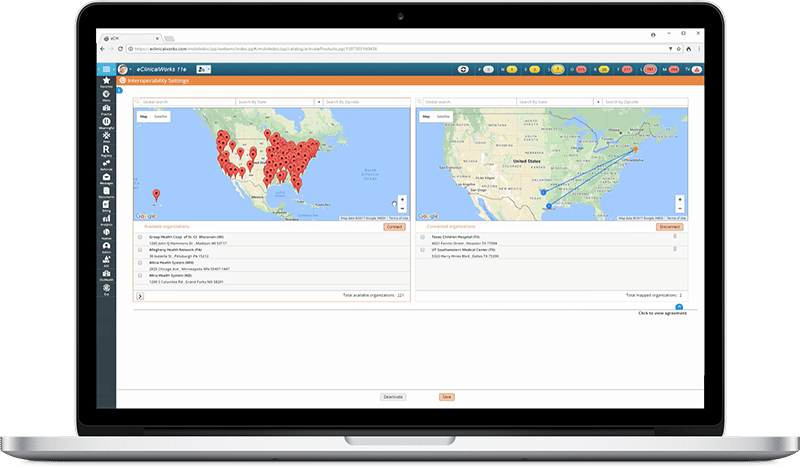
Interoperability Solutions
With nearly 50 offices and nearly 100 providers scattered throughout Southern Florida — and the need to work with dozens of hospitals — First Choice Neurology is the perfect example of how interoperability can facilitate the timely delivery of the patient information needed to improve the quality of care. First Choice’s Jose Rocha took time at the 2018 eClinicalWorks National Conference to discuss how interoperability solutions are helping this growing medical practice.
Subscribe to our podcast easily with your smartphone on iTunes®.
Brian Saal: Hello, and welcome to another edition of the eCW Podcast. Today we’re coming at you live from the eClinicalWorks National Conference here in The Music City, Nashville, Tennessee. I’m your host, Brian Saal, and with me today is Jose Rocha, Ph.D. He’s the director of Neurosciences Corporation, and they’re based out of Florida. Thank you for joining us today, it’s very much appreciated that you’re here with us. For those of you who were able to see Girish’s keynote speech yesterday, you know that there was a short film that featured Dr. Rocha, and his work with interoperability. And again, that’s why he’s here to talk with us today. One of the things that came out of that film that we saw was the desire to, well, I guess boost revenue and cut down on some costs. Can you talk a little bit about that?
Jose Rocha: Yeah. Well, the delay in getting medical records and just having them accessible, that reduces costs tremendously. But it was also we didn’t have to do an interface between us and the hospital, because they were available — the records — through the interoperability module. So, we had the opportunity to save, I think it was in the range of $30,000 because we didn’t have to do that interface.
Saal: Wow.
Rocha: Instead, the doctors are able to get everything we need from the interoperability from CommonWell and Carequality. And it has worked out great for us, because it assists us to have at a moment all of the information, from not only from the hospital but also several other providers, available to us. And it reduces the medications being tried that were already tried by the patient, or repeating procedures, having lab work that we didn’t order. So, we have all that information available. So, you know, information is key.
Saal: Absolutely. And the ability, as you mentioned, not to do repeat labs, repeat tests, that have already been done. And you can still have that data available to you, that really is a cost-saver right there.
Rocha: It is. It’s a cost savings for us and a cost savings for the patient, who doesn’t have to repeat it. And you know, we’re a neurology practice, so we have patients with memory issues, Alzheimer’s, dementia. And they don’t remember if they’ve had a test. They’ve totally forgotten about it. And they could have had it the day before, or two days ago, and they won’t remember. So, I personally find it extremely helpful to have all that information and data available so we can process the patient better.
Saal: Was there any sort of, I don’t want to call it pushback, but was there any trepidation among the providers about using this data that was coming in?
Rocha: Actually, no. I mentioned yesterday at the presentation — as far as the doctors, they love having the information. And, as far as the patients, in the 15 months that we have been live with the interoperability module, only one patient has requested to not have his information —
Saal: To opt out of the system?
Rocha: Yes.
Saal: Wow, that’s great.
Rocha: Because we work on — everyone’s opted in automatically. So, you sign the consent, and only one patient has requested not to do it.
Saal: Being based in Florida, it must be really, really helpful for you, given the number of snowbirds that you must have. I’m from Massachusetts, so I know that half of my neighborhood disappears around December 2, and reappears in April. So, having that information must be a great, great benefit to your providers.
Rocha: I mentioned that yesterday in the talk. When we originally started, we picked certain facilities that were around Florida, and we didn’t see the benefit then. And around December we started realizing, oh my God, we can get information from Massachusetts, from all these others, Boston! So we started pulling them because the patient would tell us “Oh, I had the lab work done,” and I said “Well, can you try getting it?” you know, and all that. Or, “I had the test done,” and we had all the information available to us already, and they were surprised. They were happy about it because they didn’t have to bring it with them.
Saal: In terms of ease of use, are you gathering that information when the patient is checking in, or in the room, or what’s the workflow behind that?
Rocha: Well, the workflow is — and the way we do it, because you can’t do it on demand as yet — you have to wait until the patient checks in. So, what we do is, two days before, usually, when they’re prepping the files, or the EMR chart, we actually check in the patient, pull in the information, and then put it back, depending. Just so we have the information there available.
Saal: Sure.
Rocha: And if we see something that needs more clarification, or we need to get more information, at least we can tell the patient, “Can you get us the full record?” in case that didn’t come across.
Saal: Recently, I had the opportunity to talk with one provider who was concerned about information overload, that they would be given too much information that is coming in for them to act on it appropriately. Have you or your providers ever experienced that?
Rocha: There was actually a question about that yesterday, and I think it happens, but you have the information to view, you import into the EMR, into your EMR, what you want. So, it’s what’s relevant to you. I mean, I can see a patient’s immunizations, which I don’t care about. It’s not something that’s important to me, so I don’t import that part. But radiology reports, lab reports, those things are important to us, so those get imported.
Saal: It’s interesting because earlier on we had heard the same sort of trepidation about being able to go out and get our ex-histories, where you were going to be pulling in this mountain of data about scripts. And in the end, folks found out that they would only take what they wanted and leave the rest behind. So…
Rocha: That’s basically it. All the information comes up, and then you choose what you want, and you make that part of your record. The other part is not part of your record.
Saal: How difficult was the implementation?
Rocha: Uh, click, click, click! That was basically it. I mean, the only part that basically we had to do, is pick which facilities we wanted records from. And yesterday I think we had Farah, from your team, share some statistics that we’ve received 35,000 documents from outside facilities just last month.
Saal: 35,000 documents in 30 days? That’s really astounding.
Rocha: Yes, so that’s just incredible the amount of information and data that we’re getting from. It’s just saving us a bunch of time, from having to request medical records, or pull out reports, or be running and calling this doctor or that doctor.
Saal: And having them faxed, and having to collate them. That all takes time, and I definitely can understand in a neurology practice where you’re dealing oftentimes with emerging situations, time is a super factor, a very, very big factor.
Rocha: One of the stories that I was telling you is we had a patient who came to the hospital and was a stroke patient. And we didn’t have any information on the patient, so one of the doctors decided, let me see if I can get some information from eClinicalWorks. So, this is a patient in the hospital. And he went into eClinicalWorks, created an appointment, and pulled records, and realized that the patient had records from Cleveland Clinic and other places, and I’m thinking, and so, a month later, I’m looking at an appointment that has no charges, no nothing! I look at the log. It’s created by a doctor, and I’m like, “A doctor?!” And I go and I ask him, what happened here? And he told me, well, there was a patient that came in with a stroke, I need to know some information, and I used it. And I’m like, oh, OK, alright, did that help? OK. But it was just a tool being used.
Saal: And it shows again, as I was saying, the need for speed, if you will, of getting that information, particularly when we’re talking about a stroke victim. That’s just a great story. This is a really silly question, but I’m going to ask it anyway: Would you recommend the interoperability solution that eClinicalWorks has to other users?
Rocha: Definitely. I mean, it’s free, so there’s no charge for it. The setup is click, click, click, you know? It provides you a more complete view of your patient. I can’t imagine. One of the things that me and the crew I’m here at the Conference were asking to each other: Why wouldn’t somebody do it? I just find it helpful information and there’s no cost.
Saal: That’s actually probably the better question. I should have asked it that way. Why wouldn’t somebody actually go out and be able to gather that information which, as we say, could be so, so helpful for patient care, and provider sanity as well?
Rocha: I mean, you always want to make sure that you have the best view of the patient, the most complete view. We talk about being a holistic kind of treatment, you know? So, being able to see everything that’s available out there for the patient that might be relevant. And what’s not relevant? Just don’t make it part of your record, you know? But you never know, there’s a lot of things that could be relevant that the patient might not know, or forget.
Saal: Well, thank you so much for being with us this afternoon, Dr. Rocha. It’s been a real pleasure talking to you. I found that story about the stroke patient absolutely fascination. So, again, thank you very much for joining us.
Rocha: Thank you. My pleasure.
Saal: And if you’d like to see more eCW Podcasts, you can find them on iTunes, YouTube, and, of course, on my.eclinicalworks.com. My name is Brian Saal, and if you’re here at the National Conference, please enjoy the rest of the Conference, and certainly enjoy our Music City Celebration tonight! If you’re not, I wish you all well and take care. Thanks for joining us, bye-bye!
